















Abstract:Introduction: Osteochondromas rarely grow from flat bones like scapula and pelvis. These tumours grow in sync with the growth of the child. They usually involve the growing ends of long bones, more commonly the distal end of femur.
Case report: We report a 15-year-old boy presenting to us with an osteochondroma of the iliac wing. It was of a rare sessile variant. The tumour was causing him extreme pain and mechanical block to squatting, sitting cross-legged and walking. The tumour was surgically removed by extraperiosteal resection. The patient was followed-up for one year. He did not suffer from a recurrence or symptoms of pain or weakness after one year.

Conclusion: Pelvis forms an unusual site of presentation for an osteochondroma. These tumours, should they arise from the pelvis are notoriously dangerous as they may cause compression of lumbar nerve roots. Complete removal of these tumours extraperiosteally gives a drastic relief to the patient’s symptoms. Patient should be followed up carefully to look for recurrence of this tumour.
Introduction: Osteochondromas are common benign tumours seen in the metaphysis of long bones.[1] They usually seen in the second decade of life and grow during the adolescent growth spurt. [1, 2] These tumours cease to grow after growth maturity. The most common complaints of patients with osteochondromas are pain, swelling, cosmetic deformity, limitation of movements of adjacent joints. We report a case of a 15-year-old boy diagnosed with an ostoechondroma arising from the iliac wing.
Case report:
A fifteen year old boy presented to our outpatient department with complaints of solitary swelling over the right pelvis. She was apparently normal two years back when she noticed a small swelling over the right pelvis two years back. The swelling progressed to the current size. The swelling caused her pain while walking for long distances and climbing steps. She had a significant discomfort on lying down in the right lateral position.
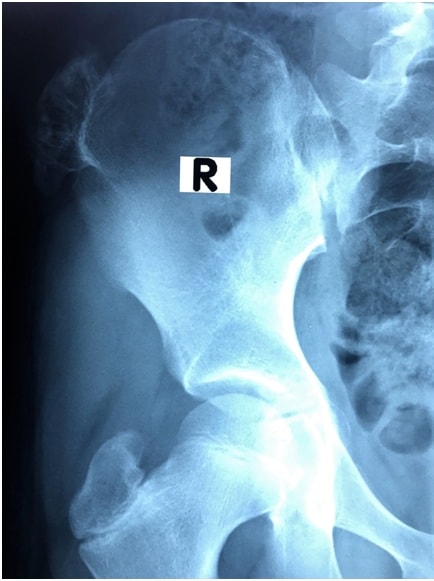
Clinical examination revealed a solitary bony hard swelling over the right iliac bone measuring around 4 x 3 cm in size. The borders were not well defined. There was no local rise in temperature or skin changes visible over the swelling. He was screened for similar swellings in the body and none were found. The swelling was fixed to the iliac bone. Radiographs of the pelvis revealed a solitary sessile osteochondroma arising from the outer iliac wing just below the iliac crest.
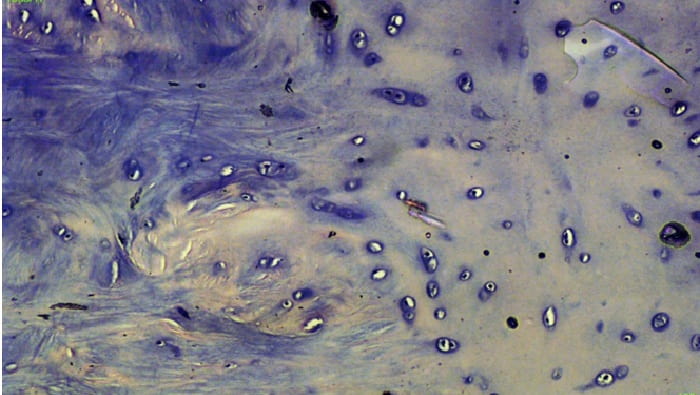
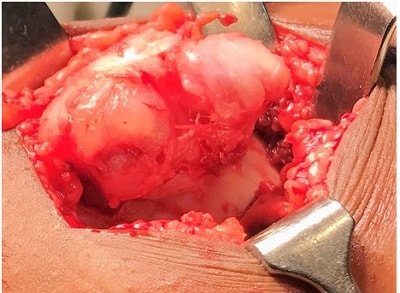
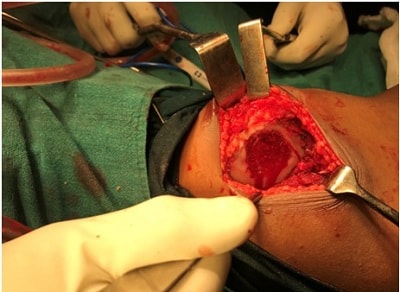
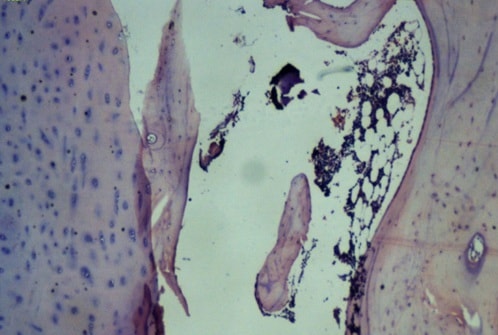
The tumour was completely excised by extraperisoteal resection. Precautions were taken not to damage the outer table of the iliac bone. The excised tumour was sent for histopathology studies, which confirmed the diagnosis of osteochondroma. Macroscopy showed bony fragment with soft tissue attachments of size 4x3x1 cm. Microscopy revealed multiple sections of bone fragments with a cartilaginous cap with trabecular bone and fatty Stissue.
Discussion:
Osteochondroma form 43.7% of all bony neoplasms [1]. The incidence of these tumours in males to females is 1.6-3.4:1 [1, 3] The most common site of osteochondroma is distal femur [4] Osteochondromas of the iliac bone are extremely rare. They form about 5% of all osteochondromas occurring in the human body. [5] They are developmental lesions of the bone rather than primary bone neoplasms. The inactivation of the tumour suppressor genes EXT-1 is required for osteochondroma to occur. [6, 7]
 The most commonly agreed cause for osteochondroma to occur is iatrogenic injury to the growth plate usually secondary to surgery or irradiation. [8, 9] Virchow, Muller and Keith’s theories have explained the origin of osteochondromas as well. [10].
The most commonly agreed cause for osteochondroma to occur is iatrogenic injury to the growth plate usually secondary to surgery or irradiation. [8, 9] Virchow, Muller and Keith’s theories have explained the origin of osteochondromas as well. [10].
Pelvic osteochondromas are rare and are usually asymptomatic. Pelvic osteochondromas can compress the lumbar nerve roots, which then have to be surgically excised [11, 12, 13]. Our patient did not have symptoms of lumbar nerve root compression, but had severe pain while squatting and sitting cross-legged. Pedunculated osteochondroma (88.2%) are more common compared to sessile variants. [2] our patient had a sessile osteochondroma, which further adds to its rarity.
These tumours are rarely malignant. About 1% of all osteochondromas become malignant lesions namely chondrosarcoma. [1] About 5% of hereditary multiple exostoses become malignant [1] Sessile, multiple osteochondromas are usually at high risk for malignant conversion. The height of the cartilaginous cap is also a sensitive indicator for malignancy. Cartilage caps thicker than 2cm are at high risk for malignancy and should be approached cautiously.
Plain radiographs are usually sufficient to diagnose osteochondromas. The most consistent findings are a pedunculated or sessile bony outgrowth that extends to the medullary cavity. Pedunculated exostosis are more commonly seen.. Computed topography usually reveals the extent and size of the tumour. MRI aids in demonstrating the thickness of the cartilaginous cap. A cap thickness of more than 2cm increases the propensity of the tumour to become malignant. [2, 10, 11, 12] Definitive diagnosis is usually by histopathological examination. Cortical and cancellous bone is seen continuous with the corresponding components of the parent bone covered by a hyaline cap which is usually diagnostic.
Most tumours are asymptomatic and can be treated by observation and educating the patient about warning signs of malignancy. However if there is a clear hindrance in performing daily activities like difficulty in walking, sitting, squatting or movement of his joint along with severe pain, such as our patient, an en bloc excision procedure might be opted for as treatment of choice. Pelvic osteochondromas involving iliac bone have been reported to cause lumbar nerve root compression.[2, 13] Pubic symphysis osteochondromas have known to cause bladder outlet obstruction. [2, 14]
The presence of neurovascular deficit due to the tumour, a pathological fracture and a sudden spurt in the growth of the tumour are absolute indications for surgery. The cartilage cap must be completely excised to avoid recurrence of the tumour. Our patient has severe pain while walking, squatting and lying down. The tumour was therefore excised en bloc. Our patient was followed up for one year. There has been no evidence of recurrence of the tumour and our patient is pain free and able to perform all her daily activities without pain.
Conclusion:Osteochondroma of the iliac wing are rare tumours. They usually present with a cosmetic deformity and pain. The treatment of these tumours is extraperisoteal excision. Excision usually demonstrates good results and symptomatic relief.
Clinical message:Pelvis forms an extremely unusual site for presentation of osteochondroma. Sessile variants are even rarer such as our patient. These tumours are asymptomatic but can cause compression of lumbar nerve roots, mechanical block to activities like sitting cross-legged, squatting or walking. Such patients recover well with excision of the tumour.
Author 1: Dr Supreeth Nekkanti
IORG Membership number: IORG-AM-175
Author 2: Dr Sagar Savsani
Junior Resident
Author 3: Dr Yuva Chandan Reddy
Affiliation:Department of Orthopaedics
JSS Medical College, Mysore
Author 4: Dr Archana Meka
Affiliation: Department of Dermatology, JSS Medical College, Mysore
JSS Medical College and Hospital
J.S.S. Medical College, Mysore, was started in 1984-85 and is imparting education in medical sciences (MBBS) course. It is recognized by the Medical Council of India. It has now become a constituent college of JSS University established under Section-3 of UGC Act from 28-05-2008. It is recognized by The General Medical Council, Sri Lanka Medical Council and WHO. The hospital has state-of-the-art infrastructure and the most advanced equipment. It is a non-profit hospital and is dedicated to serve the poor and downtrodden with affordable and quality healthcare.
The new JSS Hospital facility with 1,800 beds under one roof is one of India’s biggest hospitals. It provides service in 37 specialities/super specialities and has 55 special clinics. It caters to the healthcare needs of more than 16,000 outpatients in addition to the existing number of 18,000 and 3,500 inpatients every month.

References:
1. Sharma, N Kalsotra, P Gupta, I Wani, M Singh, D Singh. Solitary Osteochondroma Of The Ilium: A Case Report. The Internet Journal of Orthopedic Surgery. 2009 Volume 16 Number
2. Prafulla Herode¹, Abhijeet Shroff¹, Pranav Patel¹, Pallav Aggarwal¹, Vishal Mandlewala¹ A Rare Case of Pubic Ramus Osteochondroma Journal of Orthopaedic Case Reports; Volume 5 (3) July – Sep 2015 51-53
3. Wodajo FM. Cartilage Lesions. In: III PT, Einhorn TA, Damron TA, editors. Oncology and Basic Science. 7th ed: Lippincott Williams & Wilkins; 2008: 132-5.
4. Robert K. Heck J: 20. In Campbell’s Operative Orthopaedics. 2. 11th. S. Terry Canale JHB. Philadelphia: Mosby Elsevier; 2007:860-862.
5. Mark D. Murphey, James J. Choi, Mark J. Kransdorf et al. Imaging of
Osteochondroma: Variants and Complications with Radiologic-Pathologic
Correlation. Radiographics; 2000; 20:1407-1434.
6. Robert, D’Ambrosia, the formation of osteochondroma by epiphyseal cartilage
transplantation. Clinical Orthopaedics & Related Research; 1968 Nov;61:103-15
7. Xiao CY, Wang J, Zhang SZ, Van Hul W, Wuyts W, Qiu WM, et al.: A novel
deletion mutation of the EXT2 gene in a large Chinese pedigree with hereditary multiple exostosis. Br J Cancer 2001, 85:176-81.
8. Bone and soft tissue pathology(ppg331-335)- Andrew i.folpe, carrie y.inwardsa
volume in the series foundations in diagnostic pathology, copyright 2010 by saunders
an imprint of Elsevier,inc.
9. Cannela P, Gardini F, Boriani S. Exostosis: development, evolution and
relationship to malignant degeneration, Ital J Orthop Traumatol1981;7:293-8.
10. Variants of exostoses of the bone in children.-Randy Ray Richardson, MDSeminars
in Roentgenology- volume 40, issue-4, pages 380-390, October 2005.
11. Malghem J.Vande Berg, Noel H, et al: Benign osteochondromas and exostotic
chondrosarcomas: evaluation of artilage cap thickness by ultrasound. Skeletal Radiol
21:33-37, 1992.
12. Kreig, J. C.;Buckwalter. J. A.; Peterson, K. K.: El-khoury, G.Y.;and Robinson,R.A.:
extensive growth of an osteochondroma in a skeltellay mature patient. A case report.
J. Bone and Joint Surg., 77- A:269-273, Feb. 1995.0
13. Kim W, Kim K, Lee S, Choy W. Solitary Pelvic Osteochondroma Causing L5 Nerve
Root Compression. ORTHOPEDICS; 2009; 32(12)
14. Wang WY, Du LD, Lv WC, Tian Y, Shao Q, Zhang YH. Osteochondroma of the
symphysis pubis: a rare cause of bladder outlet obstruction. Am Surg.; 2010
Aug;76(8):916-8






{kind=link}