














Anticoagulant and anti -platelet agents are very commonly used in clinical practice. Over the past 20 years the market has been flooded with quite a few of them. There is a wide range of indication for their use and they have clear proven benefits in reducing morbidity and mortality.
It is evident from various clinical trials in medical research as to how they have been competing against one another and one’s superiority is constantly being shown over the other.
It is expected that the thrombo-embolic risk of individual patient is assessed before we embark upon such a treatment. There are various thrombo-embolic risk stratifying methods and scoring system that puts individual patient in particular risk category that helps in deciding on the most appropriate strategy for therapy for them. While the thrombotic risk is acknowledged, the bleeding risk on the other hand is less recognised or ignored.
Bleeding complications commonly occur from percutaneous procedures. Approximately 7% of percutaneous coronary interventions (PCI) performed emergently in patients with acute coronary syndrome result in major bleeding. Severe bleeding from PCI leads to significant increase in morbidity and mortality. Bleeding, as a complication of surgery may lead to substantial morbidity and mortality.
In cardiac surgery, severe bleeding occurs in approximately 7% of cases and is associated with an increased risk of post-operative mortality. Mortality rates approaching 20% have been observed in elective vascular patients with severe bleeding complications. In trauma patients, uncontrolled bleeding is the cause of between 30%-40% of all trauma-related deaths.
Newer anti platelet and antithrombotic therapy have revolutionized the medical management of patients with acute coronary syndromes (ACS) as well as those undergoing percutaneous coronary intervention (PCI). Various strategies have been adopted in using these agents that seem to have markedly reduced cardiovascular mortality and ischemic complications. However, with every strategy to reduce thrombosis, there is always the possibility of increasing bleeding complications a Yin-Yang analogy referring to opposing forces that are interconnected or interdependent in the natural world. In the case of PCI, decreasing thrombosis within the coronary vasculature may invariably increase the risk of bleeding elsewhere.

Thromboembolic and bleeding are frequent complications after valve replacement, accounting for approximately two-thirds of all valve-related morbidity… While these patients are on anticoagulant, if there are additional atherosclerotic vascular risks or atrial fibrillation (AF), low-dose aspirin (50 to 100 mg daily) is recommended as an “add-on” to life-long anticoagulation therapy. Reported data for serious bleeding complications vary from 0.5% to 6.3% per patient-year.
Perioperative management of patients on warfarin or antiplatelet therapy involves assessing and balancing individual risks for thromboembolism and bleeding. Discontinuing anticoagulant and antiplatelet therapy is usually necessary for major surgery but increases the risk of thrombotic events. Bridge therapy, the temporary perioperative substitution of low-molecular-weight heparin or unfractionated heparin in place of warfarin, is an effective means of reducing the risk of thromboembolism but may increase the risk of bleeding.
 The timing of warfarin withdrawal and timing of the preoperative and postoperative components of bridge therapy are critical to balancing these risks. Perioperative management of antiplatelet therapy requires special care in patients with coronary stents; the timing of surgery relative to stent placement dictates management in these patients
The timing of warfarin withdrawal and timing of the preoperative and postoperative components of bridge therapy are critical to balancing these risks. Perioperative management of antiplatelet therapy requires special care in patients with coronary stents; the timing of surgery relative to stent placement dictates management in these patients
Further on, perioperative management of anticoagulant and antiplatelet therapy is complicated by the paucity of randomized clinical trial data and the risk for serious adverse events. The underlying indications for anticoagulant and antiplatelet therapy vary widely, so the best approach to perioperative management is to involve all members of the health care team—hospitalist, surgeon, cardiologist, and anesthesiologist, together with the patient—to ensure that care is individualized and all relevant considerations are accounted for.

Patient and surgical risks can be identified and quantified to some extent, but patients often have greater concerns about the risk of stroke than the risk of bleeding. Ideally, nonemergency surgeries should be scheduled to allow enough time to thoroughly plan the management protocol, reducing risks for bleeding and thrombotic events as much as possible.
While much emphasis is being paid on assessing thrombo-embolic risk, we however often seem to ignore the other side of the coin that these agents can also lead to bleeding which if significant may also lead to increased morbidity and mortality. Bleeding on anti platelets and anticoagulants leads to increase in the number of hospital admission days and is also the cause for re-admission/s.
In addition this may also involve further procedures and need for blood transfusion. Blood transfusions and reoperations are used to control bleeding and avert deaths. These procedures are often costly and require large amounts of clinical and staff resources. Blood transfusions are not without considerable risks including nosocomial infection, immunosuppression, transfusion-related acute lung injury and even death.
These complications may add additional costs to the hospitalization and even post-discharge medical care . They all add up to increase patients’ stress and frustration as well as cause exponential loss of resources.
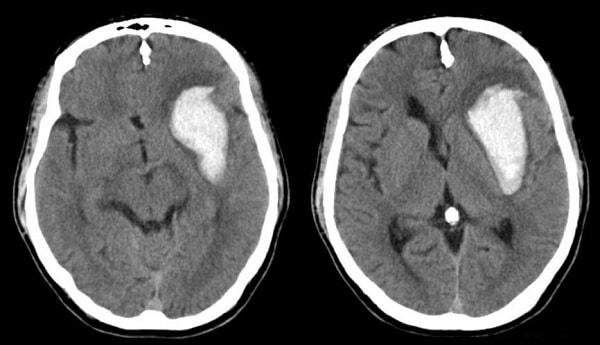
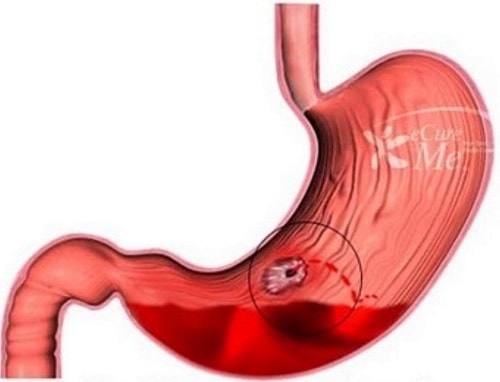
Serious bleeding can be catastrophic and can be a direct or indirect cause of death. Serious bleeding that are usually seen in clinical practice are intracranial haemorrhage and gastrointestinal bleeding. Some of these bleeding episodes are certainly preventable. However this is only possible if the anti thrombotic or anti platelet selection is adequate and appropriate. Careless use and inadequate monitoring of these can lead to serious bleeding and can become cause for litigation.
Many risk factors for bleeding with concomitant anticoagulant therapy have been identified. The assessment of bleeding risk should be part of the clinical assessment of patients before starting anticoagulation therapy, with particular attention paid to the following:
- patients who are > 75 years of age;
- those receiving antiplatelet drugs (such as aspirin or clopidogrel) or nonsteroidal antiinflammatory drugs;
- those receiving multiple other drug treatments (polypharmacy);
- those with uncontrolled hypertension;
- those with a history of bleeding (for example, peptic ulcer or cerebral hemorrhage); and
- those with a history of poorly controlled anticoagulation therapy.
With emerging newer anticoagulants where strict monitoring of the dose is not necessary, serious bleeding when occurs makes control of bleeding difficult as there are no means of assessing the degree of anticoagulation.
Until now, there has not been a simple tool applicable to the general population that can predict the risk of bleeding. Older methods for estimating risk either were derived from a low-bleeding-risk population or used variables that are not available until after treatment is begun. Currently, there are only few bleeding assessment tools i.e. HAS-BLED for AF, CRUSADE for acute coronary syndrome and IMPROVE for DVT prophylaxis. These tools are however not as well validated as the risk assessment tools for thrombo-embolism.
Keeping this mind, lately the increase in the bleeding risk in such patients is being recognised. There are now few assessment tools and scoring system in order to assess the bleeding risk of such patients. Having said that bleeding risk is still not being widely acknowledged. There is a lot of need to increase its awareness amongst health professionals as well as patients and their carers. Anti- platelet and anticoagulants therefore despite being novel treatment is like a double edged sword which the physician must choose carefully.
References
1. Ageno W, Turpie AG. Exaggerated initial response to warfarin following heart valve replacement. Am J Cardiol 1999; 84:905.
2. Aronow HD, Steinhubl SR, Brennan DM, Berger PB, Topol EJ; CREDO Investigators. Bleeding risk associated with 1 year of dual antiplatelet therapy after percutaneous coro- nary intervention: Insights from the Clopidogrel for the Reduction of Events During Observation (CREDO) trial. Am Heart J 2009;157:369–374.
3. Bertrand M, Rupprecht H, Urban P, et al. Double-blind study of the safety of clopidogrelwith and without a loading dose in combination with aspirin compared with ticlopidine in combination with aspirin after coronary stenting: The clopidogrel aspirin stent inter-national cooperative study (CLASSICS). Circulation 2000; 102:624–629.
4. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med 1998; 105:91.
5.Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation 1994; 89:635.
6. Jolly SS, Pogue J, Haladyn K, et al. Effects of aspirin dose on ischaemic events and bleeding after percutaneous coronary intervention: Insights from the PCI-CURE study. Euro Heart J 2009; 30:900–907. Oler A, Whooley MA,
7. Katholi RE, Nolan SP, McGuire LB. The management of anticoagulation during noncardiac operations in patients with prosthetic heart valves. A prospective study. Am Heart J 1978; 96:163.
8.Kovacs MJ, Kearon C, Rodger M, et al. Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin. Circulation 2004; 110:1658.
9. Levine MN, Raskob G, Hirsh J. Hemorrhagic complications of long-term anticoagulant therapy. Chest 1989; 95:26S.
10. Masters RG, Semelhago LC, Pipe AL, Keon WJ. Are older patients with mechanical heart valves at increased risk? Ann ThoracSurg 1999; 68:2169.
11. Massel D, Little SH. Risks and benefits of adding anti-platelet therapy to warfarin among patients with prosthetic heart valves: a meta-analysis. J Am Coll Cardiol 2001; 37:569.
12.Lardizabal JA, Ambrose JA et. al The balance between anti ischaemic efficacy and bleeding risk of antithrombotic therapy in percutaneous coronary intervention: a Yin-Yang paradigm.Journal of Invasive Cardiol. June 2010 22(6): 284-94
13.Oler J, Grady D. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina. A meta-analysis. JAMA 1996;276:811–815.
14. Tinker JH, Tarhan S. Discontinuing anticoagulant therapy in surgical patients with cardiac valve prostheses. Observations in 180 operations. JAMA 1978; 239:738.
15. Torn M, van der Meer FJ, Rosendaal FR. Lowering the intensity of oral anticoagulant therapy: effects on the risk of haemorrhage and thromboembolism. Arch Intern Med 2004; 164:668


