
















Use of Information Technology in Healthcare,especially Electronic Health Records (EHRs),can potentially improve healthcare. However,worldwide the usage of EHRs is limited and studies in developed countries like US have shown that electronic records systems have been slow to become part of the practices of the physicians. To gain insight into the functioning of the healthcare centers in rural India with respect to use of information technology and their fectiveness in healthcare delivery a survey was done.
Introduction
Use of Information Technology in Healthcare, especially Electronic Health Records (EHRs), can potentially improve healthcare. However,worldwide the usage of EHRs is limited and studies in developed countries like US have shown that electronic records systems have been slow to become part of the practices of the physicians. To gain insight into the functioning of the healthcare centers in rural India with respect to use of information technology and their fectiveness in healthcare delivery a survey was done.
This survey was undertaken in five taluks of Gadag district and six taluks of Bagalkot district to assess the ground realities in healthcare centers by evaluating various parameters that would influence the quality of healthcare delivery system in these districts. From the results of the survey it is evident that the quality of healthcare delivery in rural India can be improved by using information technology which will assist in apturing patient / medical records. As there were no facilities to accurately track chronicle patients’ history, the quality of referrals and hence the quality of healthcare delivery suffered.
A questionnaire consisting of a set of 86 questions related to patient load, medical record formats, hospital infrastructure and staffing information was used for this assessment. Responses to the questionnaire were tabulated. The responses were used to depict the results and draw inferences. Healthcare facilities (HC) cater to an average of 70 patients per day. The variance in this number is significant with some interior HCs catering to less than 10 patients per day and more than 100 patients per day at the Taluk Level Hospitals. Quality of healthcare depends on the efficiency of the doctors as they have to attend to at least 35 patients on an average daily. Use of health information technologies like EHRs has the potential to improve.
PATIENT RECORDS
The Medical Records Department (MRD) stores files for an average of 5 years. Data recorded regarding patients information in the Medical Records (MR) includes Name, Age, Sex, DOB, Occupation, Diagnosis and Treatment. In some cases, additional information like allergies, and food habits were also recorded. 20 HCs reported that the hospital Pharmacist maintains the medical records. In some HCs there are no full time employees for maintaining the records. Most of the HCs spend a lot of efforts (time/money) on maintaining paper based patient records.
QUALITY OF CARE
In case of paper documents the quality of information flow depended on the past history of the patient and the respondents agreed that accurate chronicle of patient history was not available in most of the cases. In both cases the quality of referral suffers that leads to repetition of the same treatment or ineffective treatment at the secondary Healthcare center. This reduces the quality of Healthcare and increases the cost of treatment.
IMPROVEMENT OF OPERATING EFFICIENCY BY USING EHRs
The study suggested that for improving quality of care, there is a need for
1. Keeping patient records that are available easily
2. Providing accurate information during patient referral to another healthcare facility
These two objectives can be achieved by employing Electronic Health Records systems.
ELECTRONIC HEALTH RECORDS
An electronic health record (EHR) is a collection of data and information gathered or generated to record clinical care rendered to an individual. It is a comprehensive, structured set of clinical, demographic, environment, social and financial data and information in electronic form, documenting the health care given to an individual.
The primary purpose of an electronic health record is for the ongoing care of the patient (orclient). The EHR should incorporate all significant clinical and administrative information pertaining to a given patient, thereby rendering it sufficient to enable the attending clinician to provide effectivecontinuing care and to determine the patient’scondition at any given time. All activities that physicians perform with paper records should be capable of being carried out using electronic records. The EHR should also enable healthcare providers other than the attending clinician to review the patient and render his/her opinion or assume the patient’s care at any time.
Secondary purposes are research/historical, epidemiology/public health, statistics, education, peer review, utilization studies, quality assurance, legal ocument (used as evidence) and healthcare policy development. The content of an EHR consists of administrative and clinical data. This content should be comprehensive and expressive thereby addressing all aspects of the healthcare process for all related disciplines and authorities. There should be no restrictions on the type of data that can be entered into the EHR.
Employable EHR
As the research is oriented towards Rural ndia, there is a need for using a simple and pragmatic EHR which excludes non-essential ata. This kind of simplification will aid in motivating people – doctors, technicians and atients – to use this EHR. The EHR so esigned is called an Employable EHR (EEHR). The following sections provide etails on the Employable EHR.
The administrative content includes
1. Identification – Patient’s full name, Medical record number, Address, Mother’s maiden name
2. Lifestyle indicators – Education level, rofession, allergies, chronic illnesses, Marital status, Food type, smoking, alcohol
The clinical content includes
1. Complaints, Physical examination results
2. Drugs prescribed, inpatient history
3. lab reports: pathology / radiology / ECG / EEG / EMG
1. Next of kin/guardian
2. Financial data
3. Race
4. Cost indicators
5. Workloads of care providers
6. Productivity and performance of care roviders
7. Comparison with standards of care
8. Birth & Death related data
WebEHR system
The system designed to implement the usage of Employable EHR is called WebEHR.
The WebEHR system:
1. Allows for the storing all of the Administrative & Clinical Content, Patient visit information, Prescription report and Inpatient & Discharge Information and reproduce them for formatted display or n paper form for study
2. Supports generation of statistical information for mining the general health onditions of public. Allows concurrent access from multiple ocations
WebEHR is capable of containing hronological information on:
1. Symptoms, complaints, healthcare requests as expressed by the patient
2. Type of events such as first visit for reatment, follow-up visit
3. Vital and common Health parameters such as: Weight, Blood Pressure, Temperature
4. Diagnosis, instructions and suggestions by reating Physician
5. Information that became available ncluding the source of such information or basis for such inference
6. Medicines prescribed by the Physician
7. Lab tests ordered by the Physician
8. Lab test results obtained from variousedical devices of a diagnostic center including reference values
9. Therapeutic interventions
10. In-patient treatment log of the patient
11. Patient’s own log of health diary
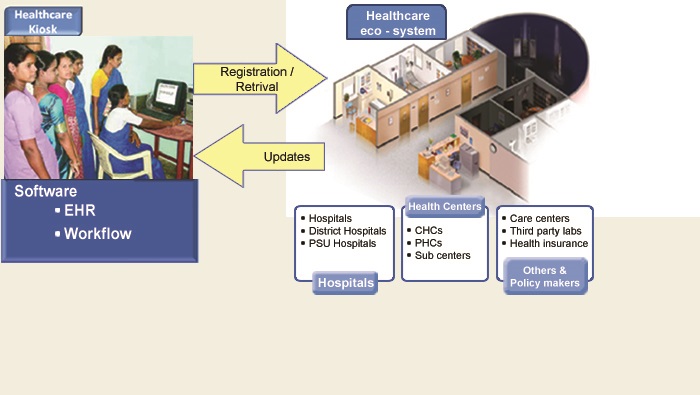
Health Kiosk
This kiosk (fig 1) will have a desktop computer with a printer connected that runs the WebEHR software.
The patient will be able to
• Register their name if it is first visit
• Take a printout of their record to the doctor.
• Doctor will examine the patient, diagnose and prescribe treatment. The doctor can also suggest for additional tests. This is done on the EHR printout of the patient.
• If additional tests are suggested the patient takes this prescription to the lab and brings the test reports back to the doctor. Doctor prescribes the treatment.
• On the receipt of the requisite diagnosis and prescribed treatment, the patient will bring back the record to the kiosk for updation of EHR.
This way the kiosk will be able to maintain the EHRs of all the patients in the rural areas. The advantage of this system is patients, doctors and other medical professionals need not know about computers and software and there is no hindrance for the EHR usage.
The system provides connectivity between the Healthcare Centers through a web-based interface. Automatic updating of the data and data storage will be facilitated by instantaneous entry of data from any given point. Subsequently, this system will provide the ability to use patient health records and statistical data for training and education of medical, paramedical, administrative personnel. This data/knowledge created will help in analysis of the health conditions for the particular demography that aids in planning for better healthcare delivery.
CONCLUSION
The benefits of implementing such a system are
• Healthcare awareness of patient increases
• Demographic information will be available for planning better healthcare delivery
• Addresses the issue of patient mobility as patient information is available for all healthcare centers as it is web enabled. No need for centralized data that reduces the confidentiality risk.
By deploying such a kiosk in different healthcare centers in rural India, we can increase the usage of EHRs thereby increasing the efficiency of Healthcare Delivery and reduce the cost of healthcare. Currently the kiosk is operational in one of the healthcare centers in Karnataka. The initial response from rural patients and doctors is encouraging.
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|



{kind=link}