
















In a five-stage process, a 120-Watt laser with MOSES technology helps eliminate nearly every remnant, while saving time and enhancing outcomes for the larger renal stones 1.5cm to 3.5cm in size, partial staghorn stones and low-volume complete staghorn stones.
The goal of kidney stone surgery has always been to remove as much of the stone volume as possible, helping the patient feel better and avoid further procedures in the future. Historically, our methods for meeting this goal began to change about 20 years ago, when ureteroscopy with holmium laser fragmentation began replacing shockwave lithoprisy. Percutaneous nephrolithotomy (PCNL) remained the preferred approach for larger stones.
Over time, holmium lasers increased in power, from as low as 40 to 80 and 100 watts. Using 100-watt holmium laser technology, we could not only fragment stones using the maximum 50Hz setting, typically with 0.3J, and retrieve the pieces through the access sheath, but also do a certain amount of dusting, or pulverizing stones into tiny fragments and washing them away during surgery.
At first, ureteroscopy was limited by rigid scopes, but the introduction of flexible ureteroscopes gave us much greater versatility, allowing for fragmentation and removal of stones at all positions in the kidneys with a simple, safe and quick access point. As more urologists adopted flexible ureteroscopy, they have in many cases replaced PCNL because the technology enabled the treatment of large or complex stones in same-day surgery with lower morbidity and fewer complications.
Four years ago, the 120-watt laser was introduced. With it, we were able to improve stone dusting,reducing procedure time even further. In my experience, procedure time has been reduced in the order of 50% over 100-watt technology. Retreatments for these larger renal stones are virtually nonexistent, whereas with the 100-watt laser, it was common to bring them back for second procedures. The recent addition of a Moses technology reduced how much the stones would move while lasing and made each pulse more impactful, thus improving overall surgical efficiency.
I have noted the Moses-only phenomenon that one of my Farmington OR nurses termed “morcellation” because the stone behaves like prostate tissue after HoLEP enucleation with the Piranha Morcellator (Richard Wolf). Using the techniques I have developed for this technology, I have cut surgery time substantially, which often enables me to add more cases each day, while at the same time enhancing outcomes for all complex cases referred to my practice.
120-Watt MOSES Laser Technology
The 120-watt holmium laser (Lumenis MOSES Pulse 120H) is a major advance that enables us to break up any stones, including very large stones greater than1.5-3.5cm, with a very low risk of bleeding,zero transfusion, and near-zero chance of injury to adjacent organs.Using the 120-watt laser and my technique, I can treat all patients in the same time as PCNL. With this approach, my patients have no nephrostomy tube. They are often out of the hospital in 1 to 2 hours, and they typically have a stent for 2 weeks.
Most colleagues in my region are doing PCNL for these larger stones. Because I am doing flexible ureteroscopy, they refer complex cases to me, such as patients with large or partial staghorn stones or small-volume staghorn stones. They also refer patients who have encountered PCNL complications like bleeding or renal hematomas that required procedure termination.
In addition, physicians refer patients who are very obese, who will benefit from supine trans-urethral treatment, instead of percutaneous removal, which is often risky in this population. PCNL is challenging for surgeons in these cases, which require special long instruments, a large table, and difficult positioning.
In the evolution of lasers, the addition of MOSES technology to the120-watt laser in recent years has taken the system to a higher plane. One of the advantages of MOSES technology is better visualization. When the stones fragment, rather than shooting away, the fragments sit nicely on the end of the fiber. We can continue to fire on the stone while it remains stable and close to the laser fiber, so we quickly and efficiently can deliver more energy. MOSES achieves this with a single modulated pulse, where a channel is first opened before the second part of the pulse pushes through.
The result is more energy is delivered to the stone, allowing much faster stone dusting and fragmentation. I see a 50 percent increase in stone ablation with the 120-watt laser, and MOSES increases it another 30 percent.
The 120-watt laser has two pedals, both of which can be customized to “dust” or “fragment” settings. This is useful on occasion in treating stones and is incredibly useful for HoLEP/MoLEP “cut” and “coagulation.”
Five-Stage Technique
Employing the current laser technology with a flexible ureteroscope, we can treat virtually any of the stones we previously reserved for PCNL. A one-stage dusting procedure is reasonable for kidney stones up to 3.5cm.My OR “cut” times range from 30 minutes for a soft, low-volume full staghorn to 2.5 hours for the largest, hardest 3.5cm stones. Larger stones might require more time, depending on their consistency, and we may choose to break that up into multiple sessions.
When I treat larger stones, I use a high-definition video flexible ureteroscope (Flex XC, Karl Storz) with a 10.7/12.7fr or 11/13fr access sheath, allowing good flow around the ureteroscope. I have a hand bulb (Utah Medical Pathfinder Plus) for irrigation. It’s important not to over-distend the collection system to avoid inducing diffuse bleeding from kidney, but I use the bulb to wash away stone dust and improve visualization. The bag is typically only 20cm in height above the patient. With these tools, I use a five-stage technique I developed to remove virtually all trace of stones.
1. Dusting –To dust the stones, I place the laser fiber maybe one millimeter away, using the MOSES “distance” setting, and paint the stone it with the laser fiber. With the patient intubated, the gentle, consistent breathing does not interfere. Depending on the hardness of the stone, I use 0.2 to 0.4 joules at 80 Hz.
 2. Stone morcellation–When a fragment breaks off, I sit on that stone,preferably in a confined space,and engage what I call stone morcellation. As the stone rolls over the end of the fiber, it gets smaller and smaller until it is completely gone. The dust washes away. This phenomenon is unique to MOSES technology and needs to be recognized and harnessed.
2. Stone morcellation–When a fragment breaks off, I sit on that stone,preferably in a confined space,and engage what I call stone morcellation. As the stone rolls over the end of the fiber, it gets smaller and smaller until it is completely gone. The dust washes away. This phenomenon is unique to MOSES technology and needs to be recognized and harnessed.
3. “Pop dusting” in the calyces– To ensure that I dust all fragments of the stones, I check all calyces. With the fiber sitting in the middle of the calyces’ semicircular structure, I can see stone fragments and pop dust them. Even in this confined space, the stones bounce around, and larger fragments roll over the fiber until they are reduced to dust.
4. Extract stone debris (take the gravel, leave the sand) – As I wash the stone dust from the kidney, I employ a basket (NCompass, Cook Medical) to sift out any larger fragments from the debris, leaving dust and tiny fragments. To this purpose, I often employ an NGage (Cook Medical) or Dakota (Boston Scientific) for the larger stone fragments.
5. Dust again– Stages 3 and 4 often need to be repeated to reduce the stone volume to under 10 percent of the initial volume.The better you become with dusting, the more stone volume washes away while you operate, minimizing the need for significant extraction, but some small fragments inevitably remain. I always finish my stone removal cycle with a final inspection and final dust until there is virtually no stone left and all that remains is about the same size as the 200uM laser fiber.
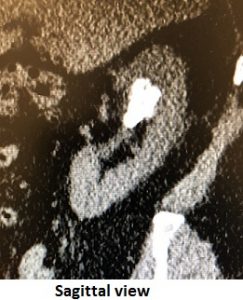
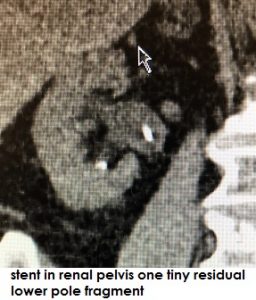 The aim of this technique is to end up with a few microscopic particles that will easily be flushed out through urination. A CT scan or ultrasound afterward will show the patient is virtually stone free, and we remove the stent after about two weeks.
The aim of this technique is to end up with a few microscopic particles that will easily be flushed out through urination. A CT scan or ultrasound afterward will show the patient is virtually stone free, and we remove the stent after about two weeks.
Advantages for Patients, Surgeons, and Hospitals
For surgeons, this procedure is faster than PCNL, as well as faster than flexible ureteroscopy with an older holmium laser. With a single access point for the upper, middle, and lower kidney, any urologist can feel comfortable dusting and removing sizeable stones from any patient. The patient’s size has no effect on ureteroscopy, so doctors don’t need to send their patients elsewhere for help. They also don’t need to take on the risks and challenges of PCNL for obese patients, or the expense of pricey disposables and overnight stays.
From the patients’ point of view, the choice between PCNL and flexible ureteroscopy with a MOSES 120-watt laser is a no brainer. With ureteroscopy, there is no nephrostomy tube sticking out of their backs. There is less bleeding and less blood in the urine, as well as a lower rate of complications, including infection. There is virtually no risk of adjacent organ injury or perinephric hematoma. Patients experience less pain and can go recover in their own homes after just a few hours.
When I talk to colleagues around the country, I find that more and more physicians are performing flexible ureteroscopy. I think techniques like mine have the potential to boost adoption of the technology even further for all stone sizes because the benefits over PCNL are so clear, and a good technique can eliminate virtually all trace of stones and do it so safely that complications and read missions are scarce.



{kind=link}