
















Selective cannulation of a small arterial branch vessel for targeted angiography or embolization is a commonly performed interventional radiology procedure, although the available toolkit of the operator may impact the ability to manage complex cases. Standard microcatheters in a pre-shaped straight or curved configuration cannot be changed or manipulated while inside the patient’s vasculature.
In the setting of complicated anatomy, such as tortuous or angulated vessels, the operator often has to perform multiple microcatheter and wire exchanges in order to select the target vessel, which can take a substantial amount of time and radiation dose to the patient and procedural staff. In some instances, if the target vessel cannot be super selected, a less targeted embolization must be performed, or the procedure must be abandoned altogether. In either scenario, the case will take longer, with implications for increased cost and resource use and the potential for complications and untoward events.
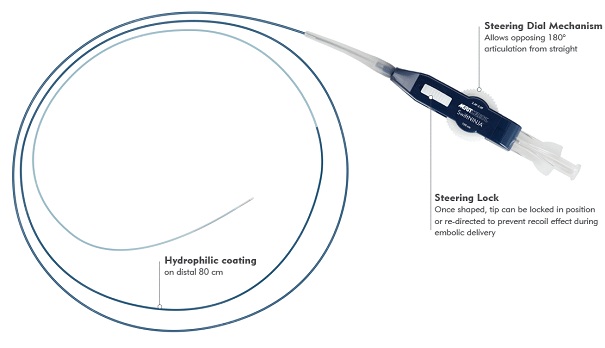
The recent availability of a steerable microcatheter (SwiftNINJA® Merit Medical; South Jordan, UT, USA) offers an alternative approach to selective cannulation. Designed with a tip that articulates up to 180° in opposing directions, this device permits in vivo steering control under fluoroscopic viewing, thusenabling rapid selection of the vascular ostium.
These characteristics theoretically facilitate faster vessel selection and shorter procedure times, and may also result in less need to open multiple instrument packs during a case. I have found all of these things to be true in cases in which I have used the SwiftNINJA.
 I recently completed a study with this device. Only limited data has been shared at this time; however,our results favored the steerable microcatheter compared with fixed-shape catheters with respect to procedure time. We also noted a cost savings associated with using the steerable catheter.
I recently completed a study with this device. Only limited data has been shared at this time; however,our results favored the steerable microcatheter compared with fixed-shape catheters with respect to procedure time. We also noted a cost savings associated with using the steerable catheter.
Below I present two cases in which use of a steerable microcatheter permitted fast, safe vessel cannulation in the setting of challenging anatomy.
Case 1
An 85 year-old man with benign prostatic hyperplasia (BPH) and severe lower urinary tract symptoms (LUTS), with an International Prostate Symptom Score (IPSS) of 29 and Urinary Quality of Life Score of 5 (unhappy), came to interventional radiology for consultation regarding management of his severe symptoms. Prostate artery embolization (PAE) was planned, as the patient’s symptoms had progressed despite medical and surgical therapy, including three transurethral resection of prostate (TURP) procedures over the prior2 years. A decision was made to perform PAE via a common femoral artery approach due to patient height and age.
After gaining right common femoral artery access, a 5-French modified Uterine Artery Catheter (mUAC, Merit Medical; South Jordan, UT, USA) was used to access the left internal iliac artery . Left internal iliac angiography demonstrates a common trunk of the superior and inferior vesical arteries (red arrow denotes the left prostatic artery).
The left prostatic artery was selected with the SwiftNINJA steerable microcatheter, with time to target vessel selection (microcatheter moved from tip of 5F catheter to successful left prostatic artery cannulation) of12 seconds. No guidewire was needed. A left prostatic artery digital subtraction angiography via the steerable microcatheter demonstrated successful selection of the left prostatic artery with tortuous prostatic artery branches supplying the central and peripheral zones of the prostate with no extra-prostatic enhancement.
 After initial relatively proximal left prostatic artery embolization, the steerability of the SwiftNINJAwas used to navigate through a tortuous 360-degree loop to gain more distal access into the central portion of the left hemiprostate, without the need for a guidewire . Additional distal embolization was then performed, following the “PErFecTED” technique.
After initial relatively proximal left prostatic artery embolization, the steerability of the SwiftNINJAwas used to navigate through a tortuous 360-degree loop to gain more distal access into the central portion of the left hemiprostate, without the need for a guidewire . Additional distal embolization was then performed, following the “PErFecTED” technique.
Total procedure time for bilateral PAE was less than 100 minutes and the patient was discharged home 2.5 hours post procedure. The patient’s IPSS decreased to 7 within 1 month post procedure, and his symptoms based on IPSS have remained mild for 1 year post procedure. His Urinary Quality of Life score improved from 5 to 1 (unhappy to pleased).
Case 2
An 82 year-old woman with segment 4a, biopsy-confirmed hepatocellular carcinoma(HCC) presents to interventional radiology for consultation regarding image-guided, liver directed therapy. The patient recently suffered a myocardial infarction and had to remain on aspirin and Plavix. Based on this and other comorbidities, she was not a candidate for surgical resection or ablation.
After multidisciplinary discussion, the plan was made to perform angiography and superselectivetransarterial chemoembolization of the segment 4a, left hepatic lobe hepatocellular carcinoma. After gaining right common femoral artery access, a 5-French Metarjame catheter (Merit Medical, South Jordan, UT, USA), was used to access the celiac artery.
 Celiac DSA demonstrated trifurcation of the common hepatic artery into right hepatic, left hepatic, and gastroduodenal arteries. The SwiftNINJA steerable microcatheter was used to select the left hepatic artery (LHA), and DSA images demonstrated a segment 4a branch artery (red arrow) off of the LGA supplying the tumor, with early arterial enhancement . The LHA was selected with the SwiftNINJA and no guidewire, with time to target vessel selection of 9 seconds.
Celiac DSA demonstrated trifurcation of the common hepatic artery into right hepatic, left hepatic, and gastroduodenal arteries. The SwiftNINJA steerable microcatheter was used to select the left hepatic artery (LHA), and DSA images demonstrated a segment 4a branch artery (red arrow) off of the LGA supplying the tumor, with early arterial enhancement . The LHA was selected with the SwiftNINJA and no guidewire, with time to target vessel selection of 9 seconds.
The SwiftNINJA steerable microcatheter was then used to superselect the branch artery supplying the HCC (red arrow) with prominent tumor enhancement (yellowarrow), as demonstrated on superselective angiography. The time from SwiftNINJA selection from proximal LHA to superselective branch vessel cannulation was 13 seconds, with no guidewire needed. After super selective transarterial chemoembolization, there was appropriate stasis in the feeding vessel, with no residual tumor enhancement.
The total procedure time was 45 minutes. The patient was discharged home 3 hours post procedure, and thereis no evidence of recurrence of the lesion with 9-month follow-up to this point.
Discussion
Discretionary use of the SwiftNINJA steerable microcatheter in the aforementioned cases provided seamless cannulation in situations that are typically difficult to perform. While it may seem that the steerable microcatheter is a good bailout option during cases presenting with unusual anatomy, its use before having to open a number of other instrument packs haspotential advantages. In most cases, the nonselective angiogram performed at the start of the case will reveal the presence of complex, difficult, or tortuous vessels—situations where using the SwiftNINJA would have benefits.
In my hands, having the SwiftNINJA ready to deploy has several advantages:
(1) No other microcatheteron the market canbe steered in vivo; ability to deal with complex anatomy aside, the device also lets me reach distal areas that might not otherwise be navigable.
(2) Using the steerable microcatheter avoids the use of multiple microcatheters for more complex branch vessel cannulation.
(3) As a result of 1 and 2, case times are shorter.
The steerable microcatheter has a higher unit cost compared to fixed-shape microcatheters; however, overall its overall cost depends on the case. If the higher up front cost of the SwiftNINJA avoids the use of several lower-cost microcatheters and microwires during the case, the per-case expenditure by the institution is likely reduced. Shorter procedure time lowers the impact on running a specialized angiography suite, and may also result in increased procedural efficiency and patient throughput, with higher overall procedural volumes in a given period of time.
Staff training should also be considered in the economic assessment of a new device. We found avery minimal learning curve with steering the device, but there are nuances in patient selection that may take time to fully appreciate. Once past this minimal hurdle, SwiftNINJA steerable microcatheteris easy and straightforward to adopt.



{kind=link}